What are the common symptoms of long COVID?
There are over 200 symptoms that have been reported that affect various organs in the body from the brain to the skin. Symptoms vary from person to person.
Most common symptoms include:
- Extreme fatigue
- Brain fog (problems with memory or concentration)
- Joint pain
- Changes to taste or smell
- Shortness of breath, heart palpitations and chest tightness
Other symptoms range from hallucinations, insomnia, hearing and sight changes, gastrointestinal problems to changes in periods and skin conditions².
Those that experience long COVID have described it as “a storm. One day you can have zero symptoms … then it will just go crazy and as quickly as it hits you it can go.”³
What makes some people prone to long COVID whilst others recover quickly?
The science is still out on exactly why some people suffer for longer. Persons experiencing long COVID are not thought to be infectious but one theory is that the body continues to respond to small amounts of the virus that remains in the body & become reactivated. Another theory is that the infection causes some people’s bodies to go into overdrive, attacking its own tissues.
The COVID symptom study¹ had also found that those who experienced a milder version of COVID19 are more prone to long COVID over an extended period of time.
There is evidence that the following categories of people may be more prone than others:
- Women
- Older adults
- People with pre-existing asthma
- People who had a wider range of symptoms during their initial illness
Can children get long COVID?
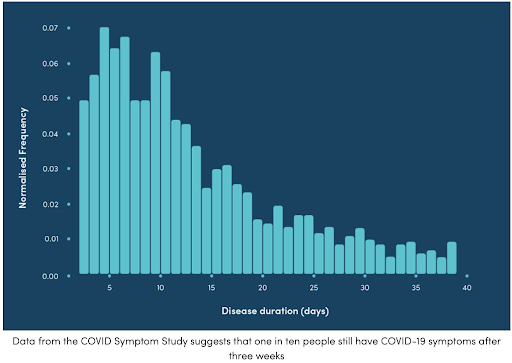
A recent study by King’s College London found that for most children, COVID tends to be a mild, short illness. The 1,500 subject study reported that the average duration of symptoms for a child is six days and fewer than 1 in 50 children are unwell after eight weeks.
How long does it take to recover from long COVID?
Recovery estimates vary but most people with long-COVID are able to live life as relatively normal. However, It is important to get healthcare advice from a trusted professional, listen to your body and rest as much as possible when symptoms flare up.
Are there any treatments available?
Large studies are underway to better understand the nature of this secondary condition. As the 216m persons infected with COVID around the world recover, their experiences help shed light on the disease.
Whilst there are no specific treatments available, the focus is on managing symptoms and enabling a slow return to normal activity.
Nutrient rich foods rich with vitamins & minerals that support the immune system are deemed beneficial and experts encourage patients to eat a holistic, well rounded diet.
Worried you may be suffering from long COVID?
If you are experiencing any new or worsening symptoms, especially 4-8 weeks post your initial COVID-19 diagnosis, speak to a doctor on oDoc. Your doctor will discuss your symptoms and if necessary, order clinical tests to rule out other causes. They will provide guidance on how to best manage your symptoms.
If you are worried or anxious about COVID19 or long COVID, speak to a mental health professional on oDoc.
Click here to download the oDoc app to your mobile device.
Sources:
- COVID Symptom Study, 2020 How long does COVID-19 last? ZOE COVID Study, UK
- Davis, H et al., (2021) Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. The Lancet
- Guardian, UK., 2020, Lingering and painful: the long and unclear road to coronavirus recovery.
- COVID Symptom Study, (2020) Do children get long COVID? ZOE Covid Study, UK
- Molteni et al., (2021).,Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2., The Lancet