
From left: CEO Heshan Fernando, Chief Growth Officer Nare Bandaranayake, Chief Medical Officer Dr. Janaka Wickramasinghe and COO Ashik Bari
Business-to-business telemedicine app oDoc on Tuesday announced it has raised $1 million in pre-series A funding. Existing investor Techstars led the investment round, along with Silicon Valley venture capital firms Hustle Fund and Unpopular Ventures. Other notable investors included Cherif Habib, Co-founder of Dialogue, a Canadian telemedicine startup with over $50 million in ARR; Vir Kashyap, Co-founder of Babajob; and LPs Bill and Leonard Lynch. “oDoc saw mass adoption across both patients and practitioners, with telemedicine being the only option for non-urgent healthcare during the lockdown.” “oDoc is taking on one of the most important problems we face — timely and affordable access to healthcare.
View Article on startuparound.com
From left: CEO Heshan Fernando, Chief Growth Officer Nare Bandaranayake, Chief Medical Officer Dr. Janaka Wickramasinghe and COO Ashik Bari
Business-to-business telemedicine app oDoc on Tuesday announced it has raised $1 million in pre-series A funding.
Existing investor Techstars led the investment round, along with Silicon Valley venture capital firms Hustle Fund and Unpopular Ventures. Other notable investors included Cherif Habib, Co-founder of Dialogue, a Canadian telemedicine startup with over $50 million in ARR; Vir Kashyap, Co-founder of Babajob; and LPs Bill and Leonard Lynch.
Founded in 2017 by Heshan Fernando (CEO), Nare Bandaranayake (Chief Growth Officer), Janaka Wickramasinghe (Chief Medical Officer), and Ashik Bari (COO), oDoc connects patients with doctors for video consultations and fulfils home diagnostics and medicine delivery.
Based in Sri Lanka, the app also provides a plug-and-play telemedicine solution for users. oDoc operates on a subscription model that starts at Rs 15 per user per month for unlimited video, audio, and chat consultations with doctors.
The company claims to have witnessed five times growth in revenues in 2020, while maintaining healthy unit economics.
“This growth was fuelled by the pandemic, which was a watershed for the global telemedicine industry,” the founders said in a press release. “oDoc saw mass adoption across both patients and practitioners, with telemedicine being the only option for non-urgent healthcare during the lockdown.”
The company also launched the Sri Lankan National Telemedicine Platform during the pandemic on behalf of the country’s health ministry as a corporate social responsibility project, enabling Sri Lankans to obtain free medical advice from any corner of the country.
Currently, the company has a network of more than 1,000 partner doctors, reaching out to 200,000 people, and over 65 corporate entities in Sri Lanka, India, the Maldives, and Cambodia.
“We are pleased to back Heshan and the oDoc team as they have demonstrated grit and capital efficiency,” said Shiyan Koh, Managing Partner at Hustle Fund. “oDoc is taking on one of the most important problems we face — timely and affordable access to healthcare. Consumers’ willingness to use digital health solutions has only accelerated during the COVID-19 pandemic and we see multiple paths to growth here.”
View Article on myfinancial.tech
From left: CEO Heshan Fernando, Chief Growth Officer Nare Bandaranayake, Chief Medical Officer Dr. Janaka Wickramasinghe and COO Ashik Bari
oDoc, Sri Lanka’s leading digital health company, announced it had closed $ 1 million in pre-series A funding at double its previous valuation.
The funding will be used to create a seamless customer experience across the healthcare and insurance verticals in the region.
Existing investor Techstars led the investment round along with leading Silicon Valley venture capital firms, Hustle Fund and Unpopular Ventures.
Other notable investors included Cherif Habib (co-founder of Dialogue, a Canadian telemedicine start-up with over $50M in ARR), Vir Kashyap (co-founder of Babajob) and LPs Bill & Leonard Lynch.
The investment will be used to expand operations and create a seamless customer experience across the healthcare and insurance verticals in the region.
Founded in 2017, the company connects patients with doctors for video consultations and fulfils home diagnostics and medicine delivery. The company grew revenues by 5X in 2020 whilst maintaining healthy unit economics.
This growth was fuelled by the pandemic, which was a watershed for the global telemedicine industry. oDoc saw mass adoption across both patients and practitioners, with telemedicine being the only option for non-urgent healthcare during the lockdown.
During the pandemic, the company also launched the Sri Lankan National Telemedicine Platform on behalf of the Ministry of Health in Sri Lanka as a CSR project, thus enabling any Sri Lankan to obtain free medical advice from any corner of the county.
Hustle Fund Managing Partner Shiyan Koh commenting on the funding, stated, “We are pleased to back Heshan and the oDoc team as they have demonstrated grit and capital efficiency. oDoc is taking on one of the most important problems we face – timely and affordable access to healthcare. Consumers’ willingness to use digital health solutions has only accelerated during the COVID-19 pandemic and we see multiple paths to growth here.”
oDoc Co-Founder and CEO Heshan Fernando stated, “At oDoc, we strive to make high-quality healthcare universally accessible, affordable and personal. We are excited to transition to the next phase of growth, moving from a startup to a scale-up and thrilled to have some of Silicon Valley’s best venture builders backing us.”
With the rise of the pandemic, telemedicine services have become more critical in reducing virus contagion by reducing the need for physical waiting rooms and improving patient outcomes as other ailments and illnesses were not neglected due to missed/late diagnosis due to the fear of visiting physical healthcare hubs.
oDoc currently has a network of 1,000+ partner doctors, covering 200,000 lives and 65+ corporates across Sri Lanka, India, the Maldives and Cambodia.
View Article on ft.lk

By now, most of us have received a link to register for Sri Lanka’s mass COVID19 vaccination rollout. Whilst some of us have jumped on board, others may still be trying to decide. However, given the rumours and misinformation that are rife in society, we wanted to help our public make the most informed decision about vaccines.
In the fourth post of this blog series, we break down the results from the 200 million doses given around the world to decide whether these rumours have legs or are just misinformation.
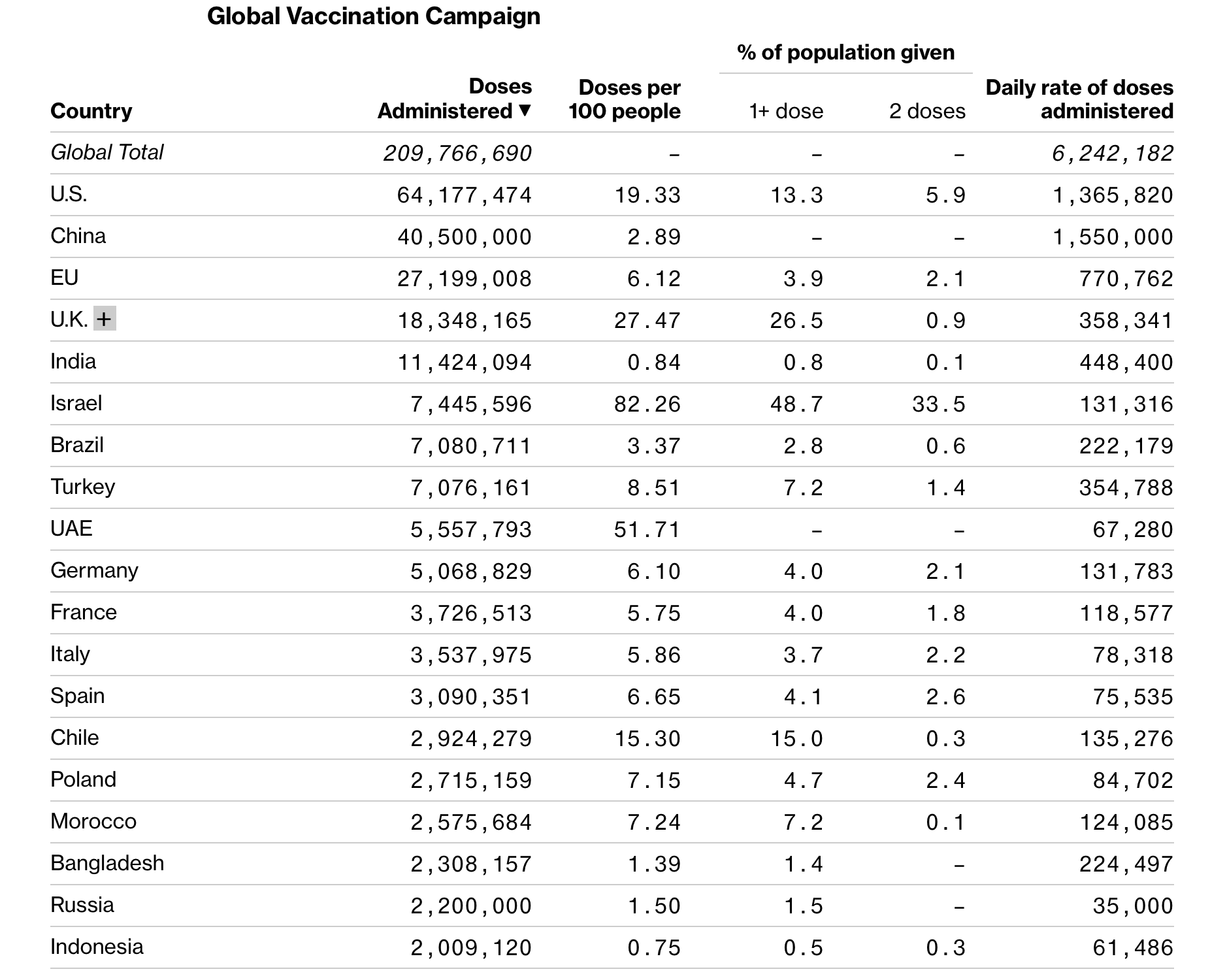
Global vaccine roll out
Globally, 200 million doses of AstraZeneca, Moderna and Pfizer/BioNtech vaccines have been administered. Some countries like Israel have raced ahead (vaccinating 71 out of every 100 people ) whilst others haven’t even started yet.
Correlation does not mean causation
Media attention on these rollouts combined with social media have resulted in widespread rumours about serious side effects or deaths due to vaccines. But what are the facts? We are talking millions of vaccinations. So even if the vaccines have a tiny 0.00009% likelihood of a severe adverse event (death or serious side effects like anaphylaxis) when the numbers inoculated are in the millions, we are bound to see one or two cases crop up. Before the agencies can investigate the event, the media publicises the cases for sensationalism without thorough fact-checking or scientific examination. The WhatsApp sharing mill goes into overdrive. What do we miss? The important principle that correlation does not mean causation.
Let us explain: Say ice cream sales increased in a certain small town, but the rate of drowning deaths in that town also increased sharply. Therefore we decide that consumption of ice cream causes drowning.
Dr Bownstein of Boston Children’s Hospital succinctly states(2) “We have to be very careful about causality,” Brownstein said. “There are going to be spurious relationships, especially as the vaccine is targeting the elderly or those with chronic conditions. Just because these events happen in proximity to the vaccine does not mean the vaccine caused these events.”
The critical question is: are these events happening at a greater rate in the vaccinated population than in the average population? To answer this question, agencies around the world investigate each event to decide what caused it.
Is anyone monitoring these vaccine drives?
The major regulatory agencies closely monitor the vaccine rollouts in each country. Before injecting a patient, vaccine centres must speak to patients and check for reasons to not inject the vaccine. Vaccine locations must also be prepared and stock supplies to treat and manage severe adverse effects like anaphylaxis.
Once someone is vaccinated in the UK, they need to stay at the location for 15 minutes to be monitored for immediate adverse reactions. The NHS uses technology for primary care providers to log all data related to each vaccination. All reactions have to be reported to the Medicines and Healthcare products Regulatory Agency (MHRA) which is then investigated. Deaths of any person who has been vaccinated are reported and investigated by the MHRA, including via post-mortem(3).
Similarly, the US CDC runs a Vaccine Adverse Event Reporting System (VAERS) which closely monitors post-vaccination adverse reactions. Since the immunisation drive began in the US in December 2020 up till January 3rd 2021, the CDC reports that 4,393 or 0.2% of the 1.8m doses administered have reported adverse reactions. Only 175 cases or 0.00009% were marked as potential severe adverse reactions for further investigation. Twenty-one of these cases were anaphylaxis which began around 13 minutes post-vaccine administration with all recovering and being discharged(4). The remainder were classified as non-serious (rash, itchy throat, mild respiratory symptoms).
But what about long term side effects?
We covered side effects extensively in our article about vaccine safety with most side effects including fever, fatigue, chills, body ache that lasts one to three days on average.
Once the vaccine ingredients do their job – aka present the spike proteins to the immune system so it can ramp up a response – the ingredients disintegrate or are broken down by that immune response. They don’t hang around in the body.
Ultimately, it is difficult to say what’ll happen in 30 years but vaccine side effects are known to happen immediately and in the short term not years later. This comes from the experience of having vaccines for 24 diseases, most of which are part of Sri Lanka’s mandatory vaccination programs for decades. Also good to note that most of those vaccine trials had less enrollments than the COVID vaccine trials.
The real risk-benefit toss up is between what appears to be a safe and effective vaccine or a deadly, unpredictable disease.
What’s happening in Israel & South Africa?
People’s hesitancy to sign up for vaccinations may be linked to partial information reported about Israel & South Africa.
Let’s look at Israel first:
Since December 19th 2020, Israel has vaccinated almost 71 out of 100 people with Pfizer/BioNTech. Priority was given to the over 60+ age group, the immunocompromised & the healthcare workers. This widespread vaccination can help scientists further validate the accuracy of the clinical trial data. Maccabi, Israel’s healthcare system, states that only 28 of the 128,600 with two doses have contracted COVID19.
However, at the same time, it appears that Israel began its third and largest peak in deaths(5) leading to its third lockdown on January 6th. So what does that mean?
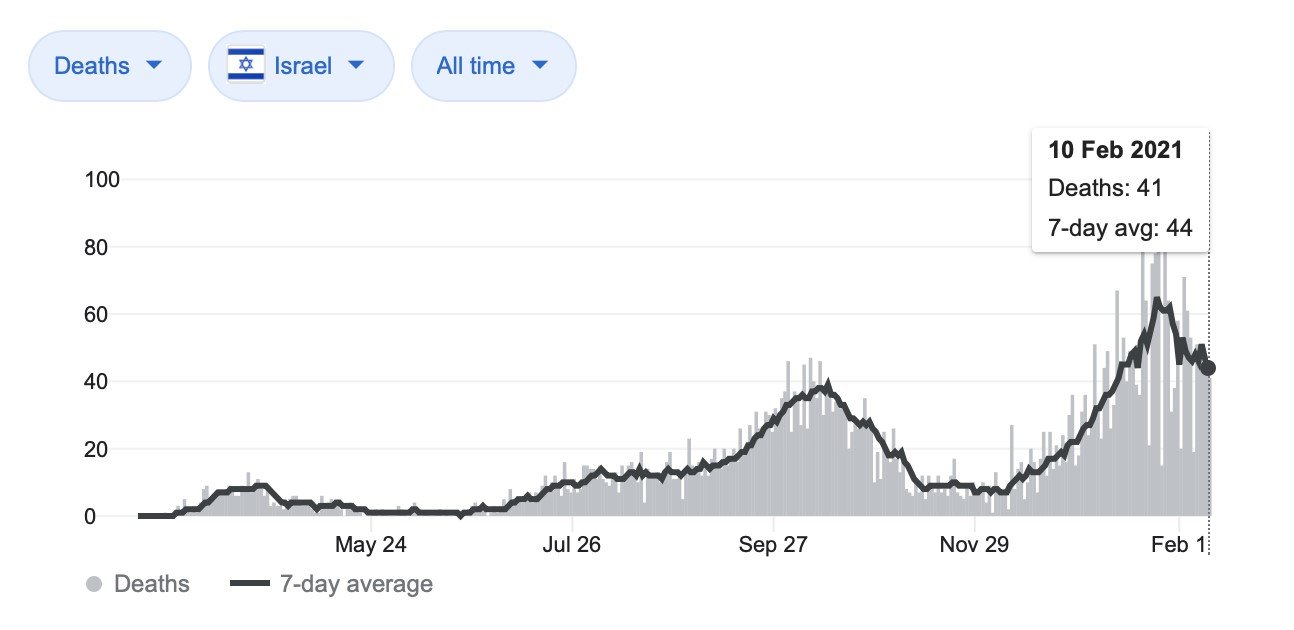
Short answer In layman’s terms: correlation does not mean causation. The overlap in time of the vaccine rollout and the increase in deaths does not mean vaccines caused deaths. It may be because deaths lag infections. The data shows less moderate to severe cases this time around than in the previous lockdown in Israel meaning that vaccines are probably helping people not fall sick!
Want more details? Read on:
Case reports suggest a trend that COVID deaths lag infections by 3-6 weeks. The spike in fatalities between December 11th and January 26th is possibly related to infections between 26th November-5th January, assuming the lower end of the lag range. The 7-day moving average of confirmed cases just before the 2nd and 3rd Israeli lockdowns look the same about three weeks before lockdown.
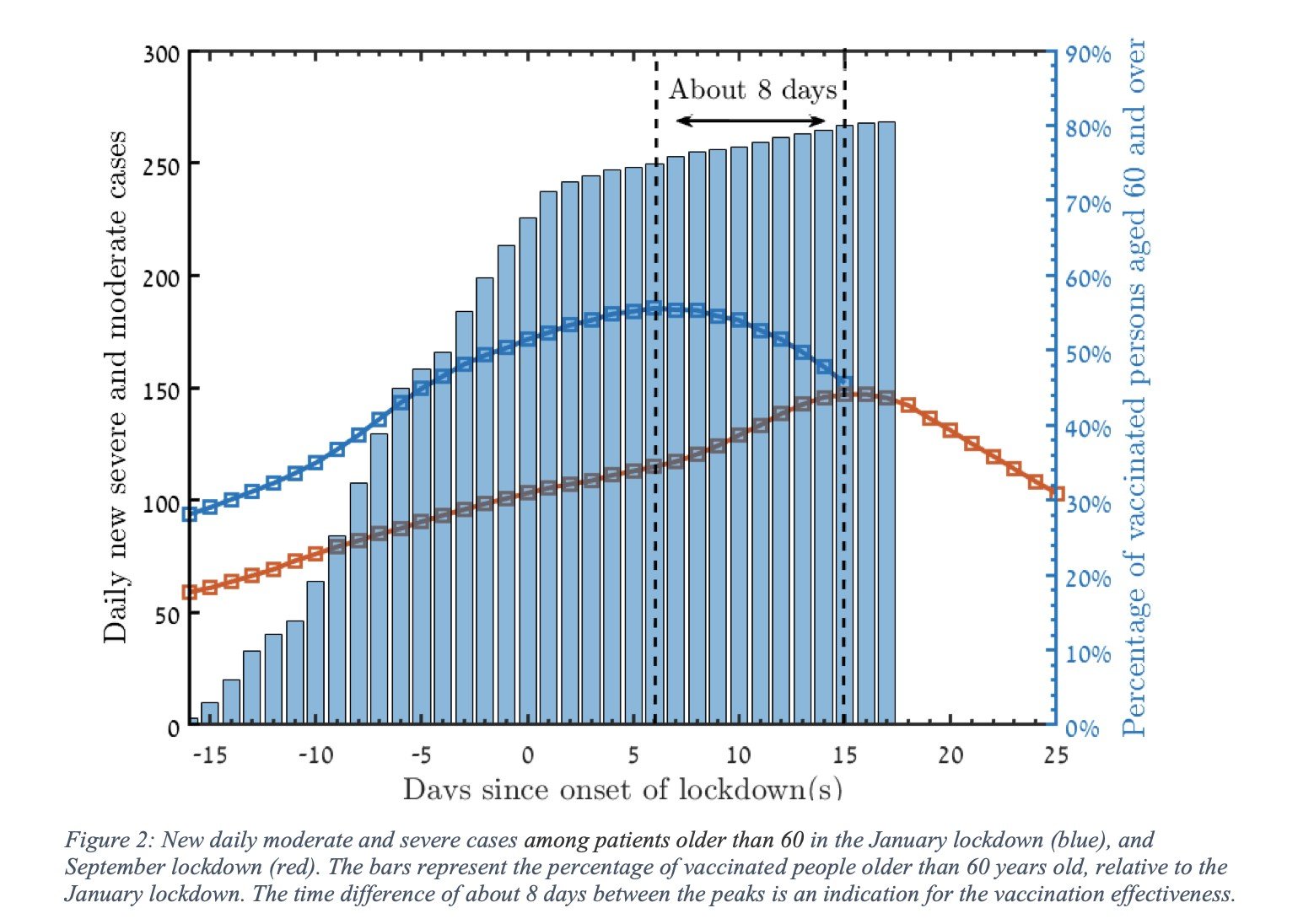
Most importantly, the number of new moderate and severe cases in the 60+ population peaked six days after the third lockdown vs 14 days after the 2nd lockdown. This earlier peak & subsequent decline is attributed to the vaccines(6).
Next, South Africa, UK & Variants:
2021 has brought great news in terms of vaccines. Still, it has also resulted in the news of variants or mutations in the Sars-Cov-2 virus that makes it more infectious. The big question has been how do the vaccines stack up against these variants?
Alongside the British/Kent variant (B.1.1.1.7), we now see news of a highly infectious South African variant (B.1.351). There is no evidence that the South African strain causes more severe illness; however, more infectious means more people infected, more severe disease, and more deaths. The South African variant’s main issue is a mutation that may allow it to dodge the immune system and render the vaccines ineffective.
As always, scientists look to prove their beliefs by conducting studies. An early study (not peer-reviewed) tested the Pfizer vaccine in the lab and have found it less effective(7). Whilst Moderna’s seem to hold up, in a 1,700 person Astrazeneca early study has shown to have “minimal” or 22% protection against mild and moderate disease caused by this specific variant(8). However, this trial was conducted on an average age group of 31 and so wasn’t created to find the efficacy on the severe disease.
However having more vaccines is now proving to be better. NovaVax, another two dose US vaccine, was found to be 95.6% effective against the original variant, 85.6% against the UK variant and 60% against the South African variant in trials.The trials against the new variants are still ongoing.
All vaccine manufacturers are working on conducting trials and creating boosters against the variants to improve effectiveness.
Finally, want to take the vaccines but have allergies?
Both The UK MHRA and the US CDC have recommended persons with histories of severe allergic reactions unrelated to vaccines or injectable medications to get vaccinated.
However, those with allergies to polyethylene glycol (PEG) or polysorbate are recommended not to get the mRNA vaccines. Furthermore, the MHRA recommends not to get vaccinated only if you have a known allergy to a component of the vaccines.
Please see the links below for ingredients of each vaccine:
To summarise, major agencies have recommended that the public get vaccinated. Only those who have known allergies to the vaccine ingredients do not get vaccinated.
How to weigh up the risk-benefits?
COVID19 has caused 2.4million deaths around the world(1) and over 400 deaths in Sri Lanka. One hundred six million people have been infected with the virus, which affects the lungs and multiple organs like the brain, heart, and kidneys, to name a few. Long COVID is a condition present in many “recovered” COVID patients. They experience fatigue, muscle weakness or body aches even six months post asymptomatic to severe illness.
Vaccines undergo rigorous clinical trials, the data reviewed by multiple panels of experts & regulators searching for efficacy and safety data. Adverse events are most likely to occur soon after vaccine administration. With over 128 million doses being administered, there have been less than 0.005% reports of severe adverse reactions. Furthermore, the vaccine ingredients disintegrate and leave your body after 1-2 days.
To put simply, COVID19 causes a more considerable risk of death and illness than the vaccines. Suppose we want to achieve herd immunity and return to economic activity (or go on holiday to our favourite locations) sooner than later. In that case, we believe it is most prudent to take both the doses of the vaccine that will be soon made available to you.
Read our previous blog on Vaccine safety: Three (scientific) reasons why they are safe
Sources
How to Keep Work Stress from Taking Over Your Life In today’s fast-paced and competitive world, work stress has become an all-too-common problem that affects

Hypertension: Everything You Need to Know Hypertension, commonly known as high blood pressure, is a chronic medical condition that affects a significant portion of the
Understanding Borderline Personality Disorder: Symptoms, Causes, and Treatment. Borderline Personality Disorder (BPD) is a mental health disorder characterised by instability in mood, behaviour, and relationships.

With the impending mass COVID19 vaccination rollout in Sri Lanka, there are murmurs about vaccines causing allergic reactions or even deaths. It was only with its mass vaccination programs that Sri Lanka could eradicate diseases like measles or polio. It remains integral to economic recovery that there is public buy-in for a COVID19 vaccination scheme.
To that end, we break down the results from the clinical trials to see whether these rumours have legs or are just in fact, misinformation.
How effective are these vaccines? Little recap from Part 1 of our Blog Series
Clinical trial data has shown that all of the vaccines authorised so far are very effective at preventing symptomatic illness. The table below gives a quick summary of the findings so far:
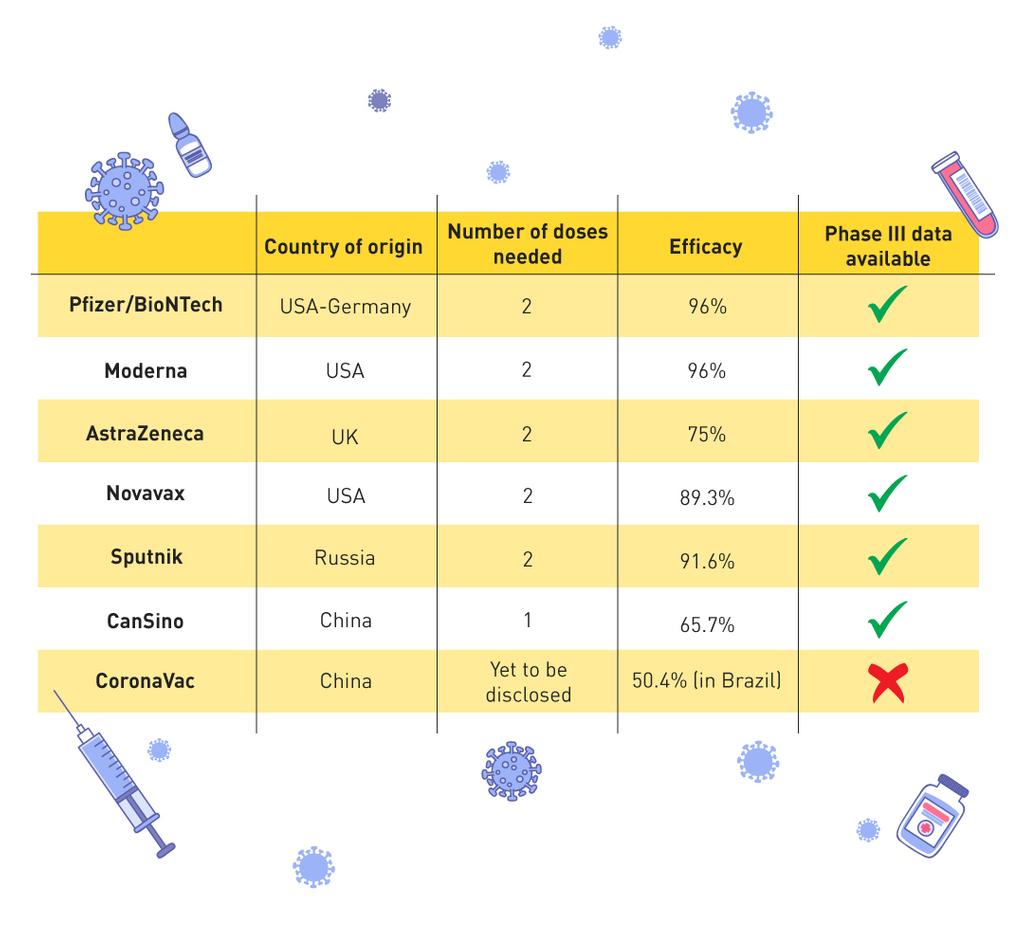
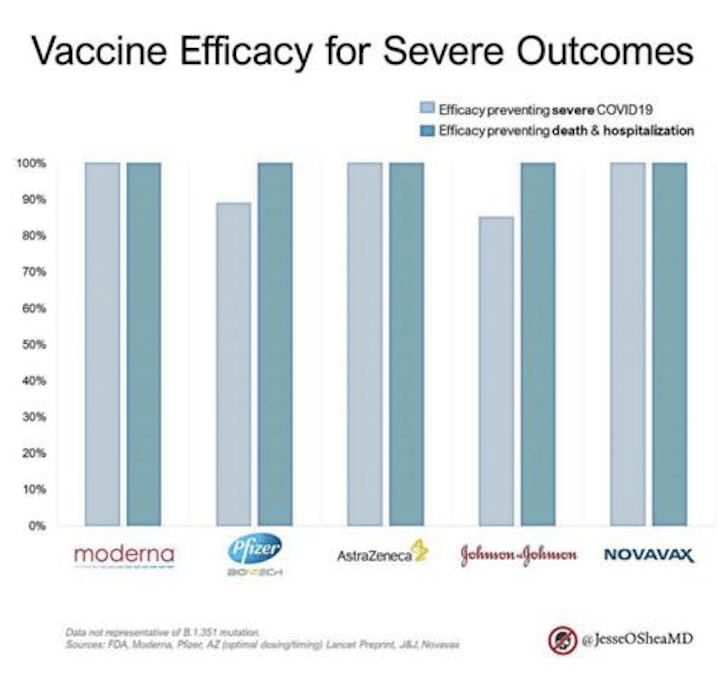
Importantly ALL the vaccines have 80%+ efficacy against preventing severe disease and 100% against deaths & hospitalisation. After 2.3million deaths around the world, this is welcome news.
1) The trials have 30-40,000 people each to mimic real-world conditions.
Phase III clinical trials are the most extensive, most time consuming and most expensive part of the development process. Scientists look to mimic real-world conditions (different ages, genders, cities etc.). They aim to see whether the vaccine effectively protects against the virus AND whether it causes any side effects in the wider population.
AstraZeneca & Moderna enrolled 30,000 people each in their Phase III, Pfizer/BioNTech 42,000, Novavax 20,000 and Russia’s Sputnik 21,000. In comparison, the GlaxoSmithKline MMR vaccine Phase III trial only enrolled 5,000 participants and is now a widely accepted part of the Sri Lankan immunisation strategy(3).
Sample sizes are large to reduce “sampling error”. Sampling error is the difference between the sampled results and the population’s results if the sample doesn’t represent the population accurately. By enrolling tens of thousands of people – each of these vaccine trials could reduce sampling error and thus be as accurate as possible in their data collection.
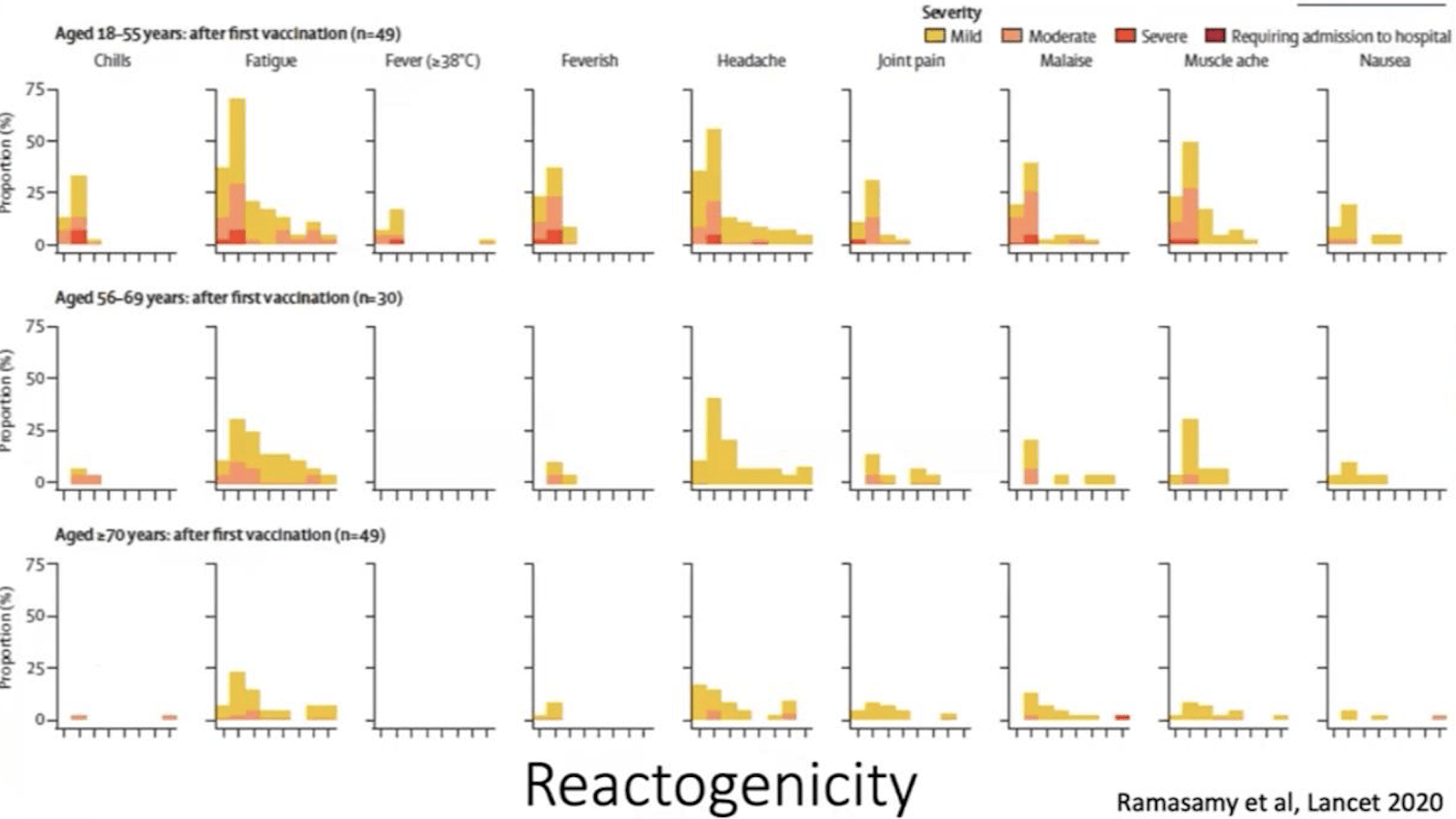
2) The trials showed mild reactions in mostly younger people which lasted a median of one day.
Every vaccine trial looks for occurrences of “local” (at the site of injection) and “systemic” (around the body) reactions to the vaccine. Local reactions include injection site pain, redness, swelling. Systemic adverse reactions include fever, fatigue, headache, chills, vomiting, diarrhoea, muscle or joint pain. If reactions occur, they happen within 1-2 days of getting the vaccine and last an average of one day.
AstraZeneca separated its participants into three age groups: 18-55, 56-69, and 70+. In the table below, we can see which local and systemic reactions occurred in the study participants and how long they lasted.
They were more common in the 18-55 age group with most complaints of fatigue, headache and muscle ache soon after getting the vaccine. For all age groups and all complaints, the reactions disappeared in a few days(4).
Pfizer/BioNTech saw younger people experiencing local and systemic adverse reactions more often and in greater intensity than the older age groups. They often felt pain at the injection site at a greater intensity than the older participants. Both groups complained of fatigue, headache and body aches.
All of Moderna’s participants complained of local reactions with pain & temporary swelling of lymph nodes being the most common. However, most reactions only lasted 1 to 2 days. Fatigue was the most commonly reported systemic reaction followed by headaches, body ache, fever and chills for 1-2 days post-vaccination.
3) The vaccines rarely caused severe adverse reactions and showed to be 100% protection against death.
As Phase III is designed to mimic the real population, events such as deaths or heart attacks that will typically occur in the real population also occur in the trial groups. The safety boards’ responsibility is to review the data to decide which events were caused by the vaccine and which occurred naturally. For this, they look at rates of these events in the general population by age group and deep dive into each case’s particulars.
None of the vaccine trials (including Russia’s Sputnik) has had a severe adverse effect resulting in death as a result of the vaccines (5)(6). Of the 84 severe adverse events (in 11,000 candidates) reported by AstraZeneca, only one classified as possibly related to the vaccine(4). This one case is 0.000085% of the total study population, a tiny percentage.
All of the vaccines peer-reviewed so far shows to have 100% efficacy against death & hospitalisation.
Weighing up the benefits
COVID19 has caused 2.3million deaths around the world(8) and over 300 deaths in Sri Lanka. None of the COVID19 vaccines reviewed thus far has yet had a death determined to result from the vaccine. Adverse events are most likely to occur soon after vaccine administration. With over 128 million doses being administered globally, there have been less than 0.005% reports of severe adverse reactions.
The choice is between contracting a virus known to cause lasting damage to the body (if not death) and taking a vaccine that is found to prevent death 100% of the time. Moreover, the vaccines reviewed thus far are not known to cause severe adverse events; the winner becomes abundantly clear.
We would urge the Sri Lankan public to accept the AstraZeneca or Pfizer vaccines.
Read our previous blog on Do the vaccines actually work?
Sources
Boo-ger season is here! Let’s begin by defining flu (short term for influenza) because it’s usually misunderstood as fever or cold. Flu is a common
As Sri Lanka rolls out its COVID19 booster program, we break down the answers to your most pressing questions. Firstly, what is a booster? A
Back to School – A Battle Between Education and COVID-19 Students are finally returning to school. But as parents, many are worried about COVID-19 safety.