සහසම්බන්ධය හේතුකාරකයක් නොවේ
සමාජ ජාලා වල පැතිරී යන තොරතුරු මෙන්ම ගෝලීය පුවත් විකාශයන්ගේ අවධානය හේතුවෙන් බරපතල අතුරු ආබාධ හෝ එන්නත් නිසා සිදුවන මරණ පිළිබඳ පුළුල් කටකතා පැතිර ඇත. නමුත් ඇත්ත තත්වය කුමක්ද? අපි කතා කරන්නේ එන්නත් මිලියන ගණනක් පිළිබඳවයි. එන්නත් මිලියන ගණනක් ලබා දී ඇති විට දරුණු අහිතකර සිදුවීමක් (මරණය හෝ ඇනෆිලැක්සිස් වැනි බරපතල අතුරු ආබාධ) ඇතිවීමේ සම්භාවිතාව 0.00009% ක් විය හැක. සිද්ධිය විමර්ශනය කිරීමට පෙර, පූර්ණ කරුණු පරීක්ෂා කිරීමකින් තොරව පුවත හෙළි කරනු ලැබේ. WhatsApp හරහා පුවත තවත් වේගයෙන් ගලා යයි. අපට මඟ හැරෙන්නේ කුමක්ද? සහසම්බන්ධය හේතුකාරකයක් නොවේ යන වැදගත් මූලධර්මය.
අපි පැහැදිලි කරමු: එක්තරා කුඩා නගරයක අයිස්ක්රීම් අලෙවිය ඉහළ ගොස් ඇති අතර එම නගරයේ දියේ ගිලී මිය යාමේ වේගය ද තියුනු ලෙස ඉහළ ගියේය. එබැවින් අයිස්ක්රීම් පරිභෝජනය දියේ ගිලීමට හේතු වන බව අපි තීරණය කරමු.
බොස්ටන් ළමා රෝහලේ ආචාර්ය බොන්ස්ටයින් කෙටියෙන් මෙසේ පවසයි (2) “හේතුව පිළිබඳව අප ඉතා සැලකිලිමත් විය යුතුය”. “එන්නත වැඩිහිටියන් හෝ නිදන්ගත තත්ත්වයන් ඇති අය ඉලක්ක කර ගනිමින් ලබා දෙන හෙයින් විශේෂයෙන් සහසබඳතා ඇති වේ. මෙම සිදුවීම් එන්නත ලබා දීම ආසන්නයේ සිදුවීම නිසා එන්නත මෙම සිදුවීම් වලට හේතු වූ බවක් අදහස් නොවේ.”
තීරණාත්මක ප්රශ්නය නම් මෙම සිදුවීම් සාමාන්ය ජනගහනයට වඩා එන්නත් කරන ලද ජනගහනයේ වැඩි අනුපාතයකින් සිදුවන්නේද යන්නයි. පිළිතුරු සැපයීම සඳහා, ලොව පුරා නියෝජිත ආයතන එක් එක් සිදුවීම විමර්ශනය කර එයට හේතුව කුමක්ද යන්න තීරණය කරයි.
එන්නත්කරණය කවුරුන් හෝ විසින් අධීක්ෂණය කරනවාද?
ගෝලීය නියාමන ආයතන සෑම රටකම එන්නත්කරණය සමීපව නිරීක්ෂණය කරයි. රෝගියකුට එන්නත් කිරීමට පෙර, එන්නත් සායන රෝගීන් සමඟ කතා කළ යුතු අතර එන්නත් නොකිරීමට හේතු සොයා බැලිය යුතුය. ඇනෆිලැක්සිස් වැනි දරුණු අහිතකර බලපෑම් කළමනාකරණය කිරීම සඳහා එන්නත් සායන සකස් කළ යුතු අතර එන්නත් වල තොගද ළඟ තබා ගත යුතුය.
එක්සත් රාජධානියේ යමෙකුට එන්නත ලබා දුන් පසු, ක්ෂණික අහිතකර බලපෑම් නිරීක්ෂණය කිරීම සඳහා ඔවුන් විනාඩි 15 ක් එම ස්ථානයේ රැඳී සිටිය යුතුය. එක් එක් එන්නත හා සම්බන්ධ සියලු දත්ත ලබාගැනීම සඳහා ජාතික සෞඛ්ය සේවය තාක්ෂණය භාවිතා කරයි. සියළුම අහිතකර බලපෑම් ඖෂධ හා සෞඛ්ය නිෂ්පාදන නියාමන ඒජන්සියට (MHRA) වාර්තා කළ යුතුය. එන්නත ලබා ඇති ඕනෑම පුද්ගලයෙකුගේ මරණ පශ්චාත් මරණ පරීක්ෂණය ඇතුළුව MHRA විසින් වාර්තා කරනු ලැබේ (3).
ඒ හා සමානව, එක්සත් ජනපද CDCය විසින් එන්නත් අහිතකර සිදුවීම් වාර්තාකරණ පද්ධතියක් (VAERS) පවත්වාගෙන යන අතර එය පශ්චාත් එන්නත් අහිතකර බලපෑම් සමීපව අධීක්ෂණය කරයි. CDC වාර්තා වලට අනුව එක්සත් ජනපදයේ 2020 දෙසැම්බරයේ සිට 2021 ජනවාරි 3 වනදා දක්වා තිබු එන්නත්කරණය හේතුවෙන් 4,393 ක් හෝ 0.2% කට අහිතකර බලපෑම් සිදු වී ඇත. වැඩිදුර විමර්ශනය සඳහා බරපතල අහිතකර බලපෑම් ලෙස සලකුණු කර ඇත්තේ එයින් 175 ක් හෝ 0.00009% ක් පමණි. මෙම සිද්ධීන් අතුරින් 21ක් ඇනෆිලැක්සිස් වන අතර එය එන්නත් ලබා දී මිනිත්තු 13 ක් අතර ආරම්භ වූ අතර ඒ කාලය තුලම පාලනය කර ඇත (4). ඉතිරි කොටස බරපතල නොවන (සමේ රෝග, කැසීම, මෘදු ශ්වසන රෝග ලක්ෂණ) ලෙස වර්ගීකරණය කරන ලදී.
නමුත් දිගු කාලීන අතුරු ආබාධ ගැන කුමක් කිව හැකිද?
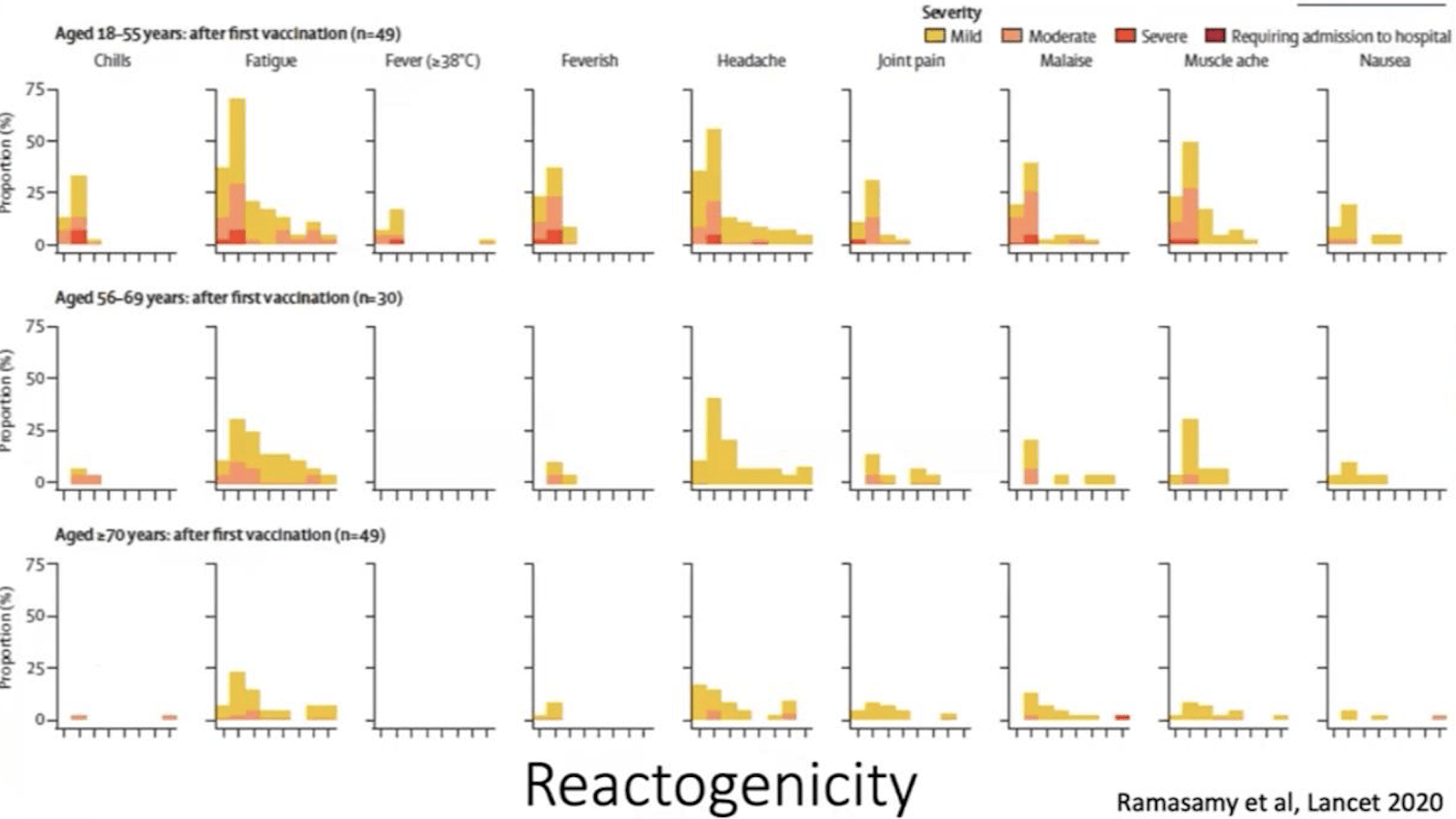
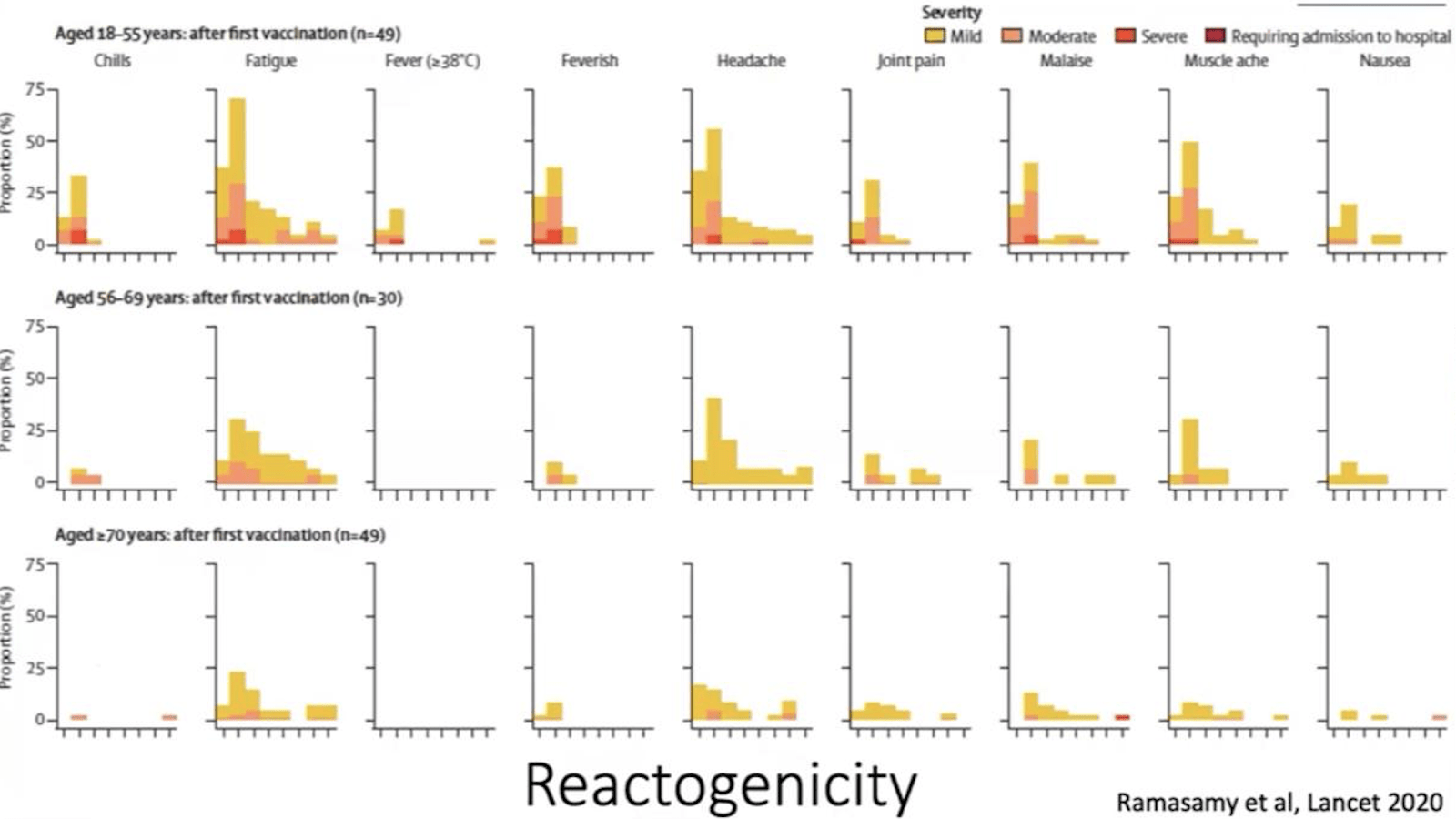
උණ, තෙහෙට්ටුව, ශරීර කැක්කුම වැනි බොහෝ අතුරු ආබාධ සමඟ එන්නත් වල ආරක්ෂාව පිළිබඳව අපගේ ලිපියෙන් පුළුල් ලෙස ආවරණය කළෙමු.
එන්නත් සංඝටක ඔවුන්ගේ කාර්යය ඉටු කළ පසු ඒවා ශරීරයේ නිදන්ගත නොවේ.
අවසාන වශයෙන්, වසර 30 කින් කුමක් සිදුවේදැයි කීමට අපහසු නමුත් එන්නත් අතුරු ආබාධ ක්ෂණිකව සිදුවන බව පිළිගත් කරුණකි. රෝග 24 ක් සඳහා එන්නත් සකසා තිබීම හා ඒවායින් බොහොමයක් දශක ගණනාවක් තිස්සේ ලංකාවේ අනිවාර්ය එන්නත් කිරීමේ වැඩසටහන් වල කොටසක් වීම හේතුවෙන් අපටද බිය වීමට කරුණු නොමැත. එම එන්නත් අත්හදා බැලීම්වලින් බොහොමයක් COVID එන්නත් අත්හදා බැලීම්වලට වඩා අඩු පිරිසක් ඇතුළත් කර ඇති බව සැලකිල්ලට ගැනීම හොඳය.
සැබෑ අවදානම පවතින්නේ ආරක්ෂිත හා ඵලදායී එන්නතක් හෝ මාරාන්තික, අනපේක්ෂිත රෝගයක් ලෙස පෙනෙන දේ අතරය.
ඊශ්රායලයේ සහ දකුණු අප්රිකාවේ සිදුවන්නේ කුමක්ද?
එන්නත් සඳහා ලියාපදිංචි වීමට මිනිසුන් දක්වන පැකිලීම ඊශ්රායලය සහ දකුණු අප්රිකාව පිළිබඳ වාර්තා වූ අර්ධ තොරතුරු සමඟ සම්බන්ධ විය හැකිය.
අපි මුලින්ම ඊශ්රායලය දෙස බලමු:
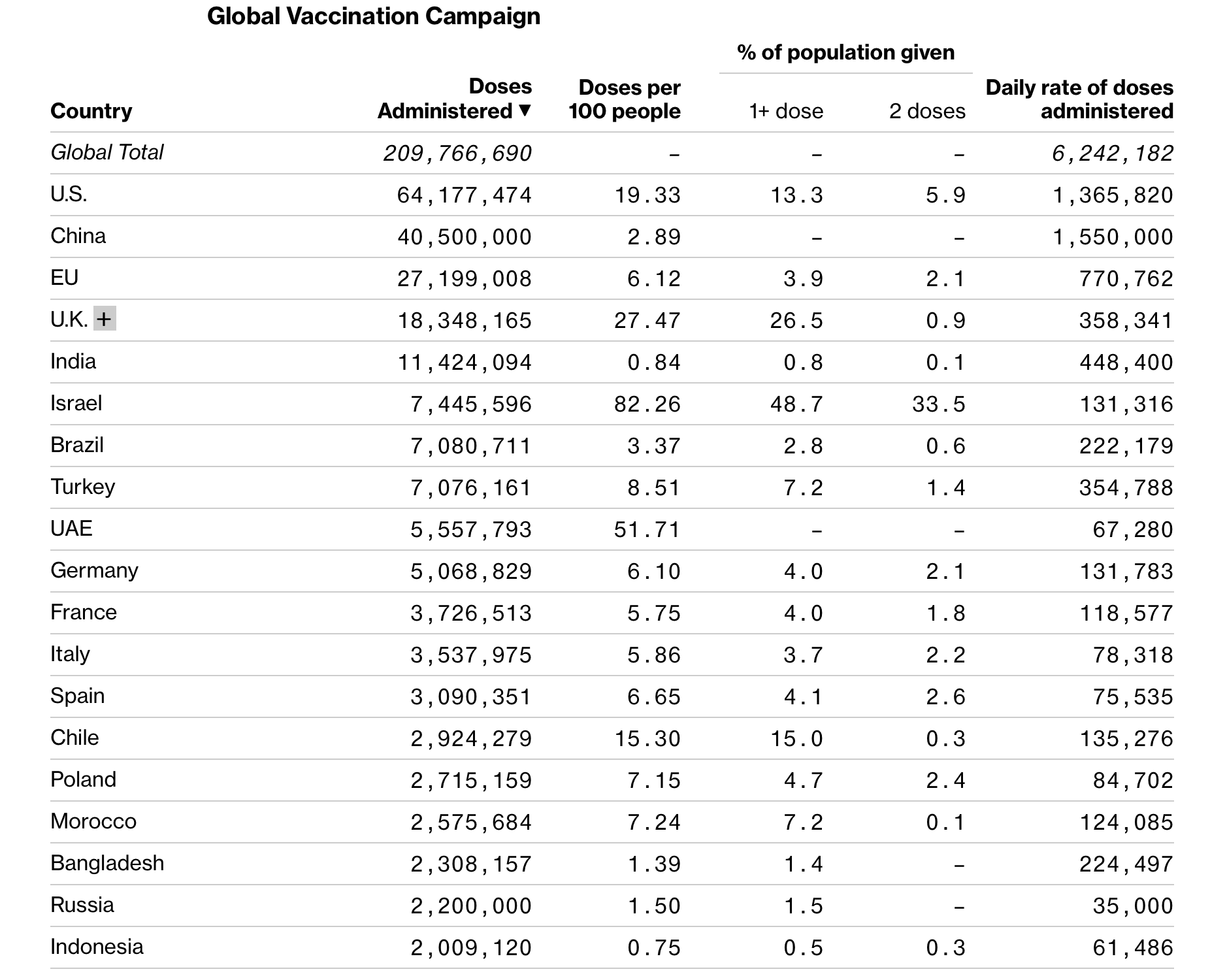
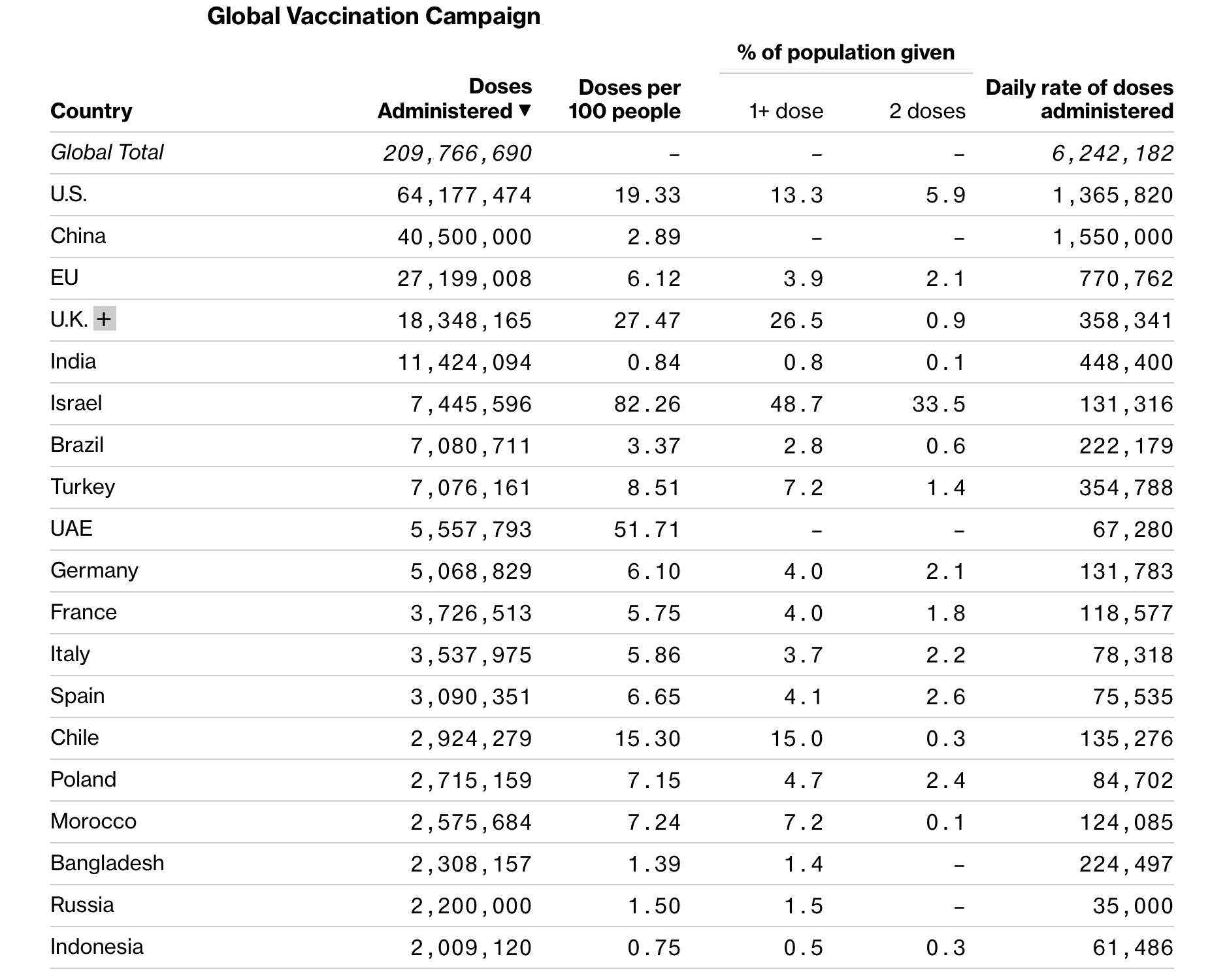
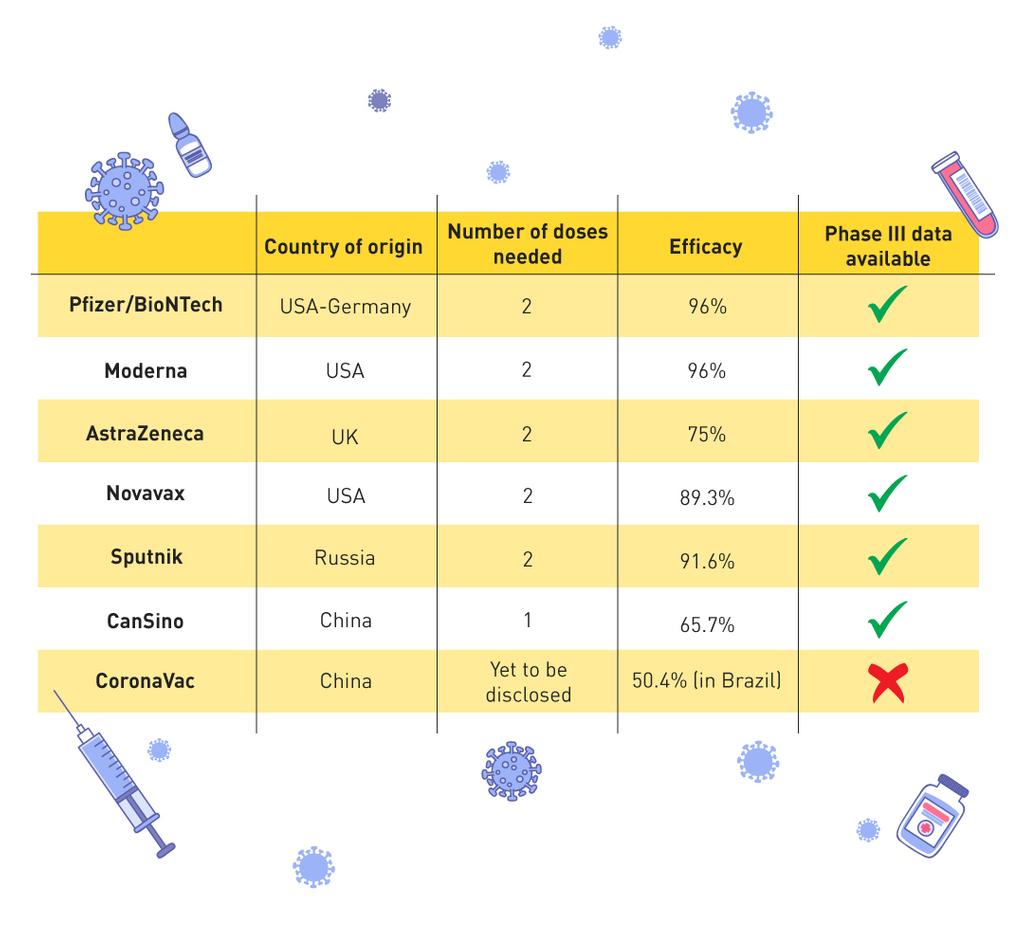
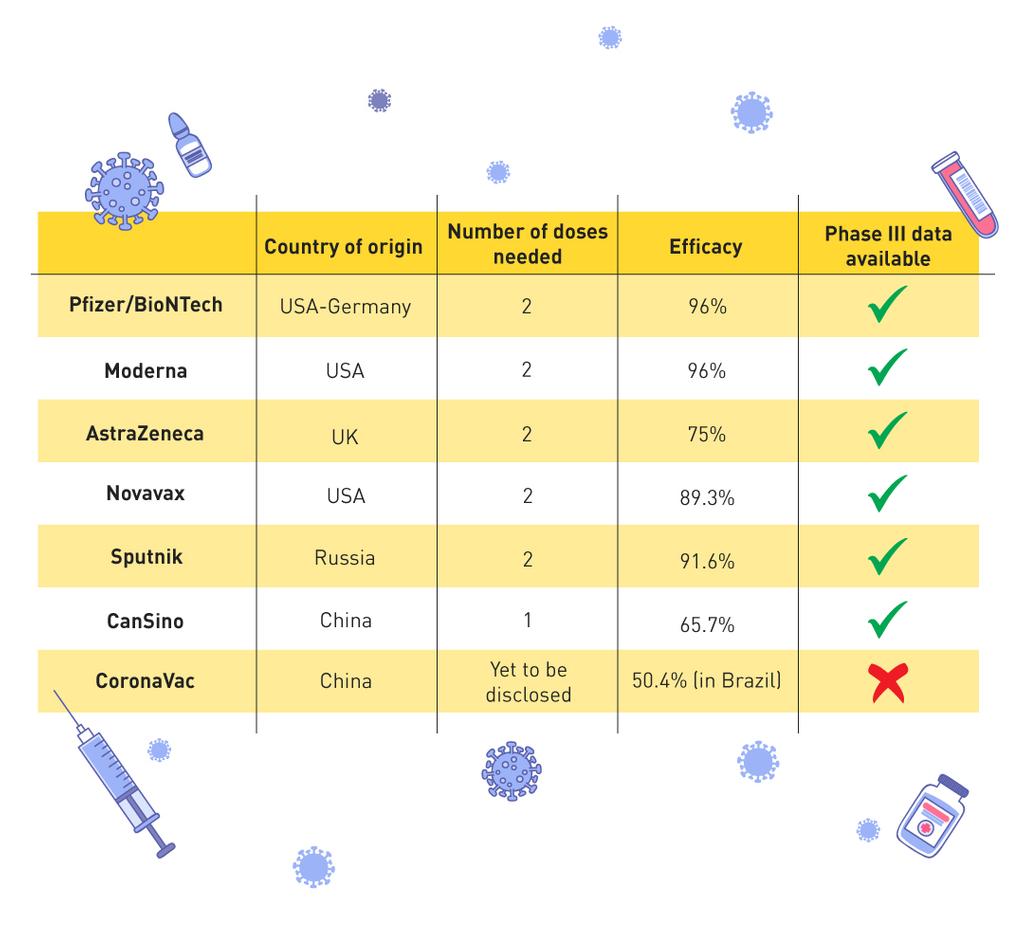
2020 දෙසැම්බර් 19 වන දින සිට ඊශ්රායලය පුද්ගලයින් 100 දෙනෙකුගෙන් 71 දෙනෙකුට Pfizer/BioTech එන්නත ලබා දී ඇත. වයස අවුරුදු 60 ට වැඩි හා සෞඛ්ය සේවකයින්ට පළමුව එන්නත් ලබා දී ඇත. මෙම පුළුල් එන්නත කිරීම මගින් සායනික අත්හදා බැලීමේ දත්තවල නිවැරදිතාවය තවදුරටත් තහවුරු කර ගැනීමට විද්යාඥයයින්ට හැකි වේ. ඊස්රායලයේ සෞඛ්ය සේවා පද්ධතිය වන මැකාබි පවසන්නේ මාත්රාවන් දෙකක් සහිත 128,600 න් 28 ක් පමණක්ට COVID19 වැළදී ඇති බවයි.
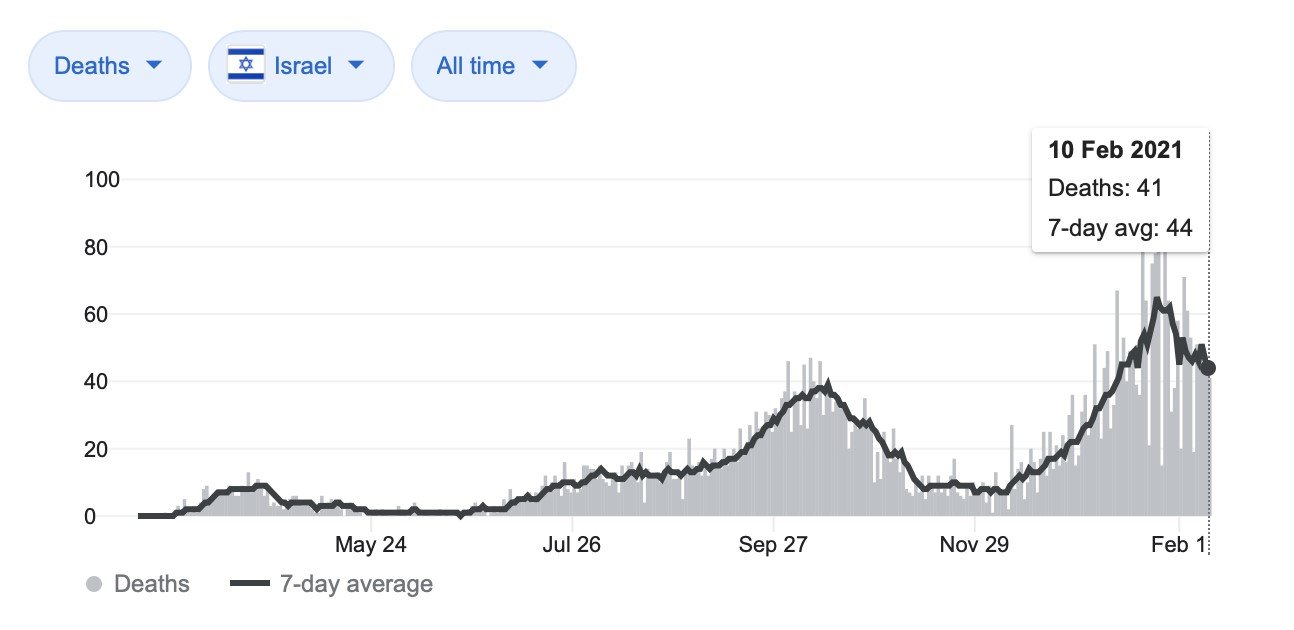
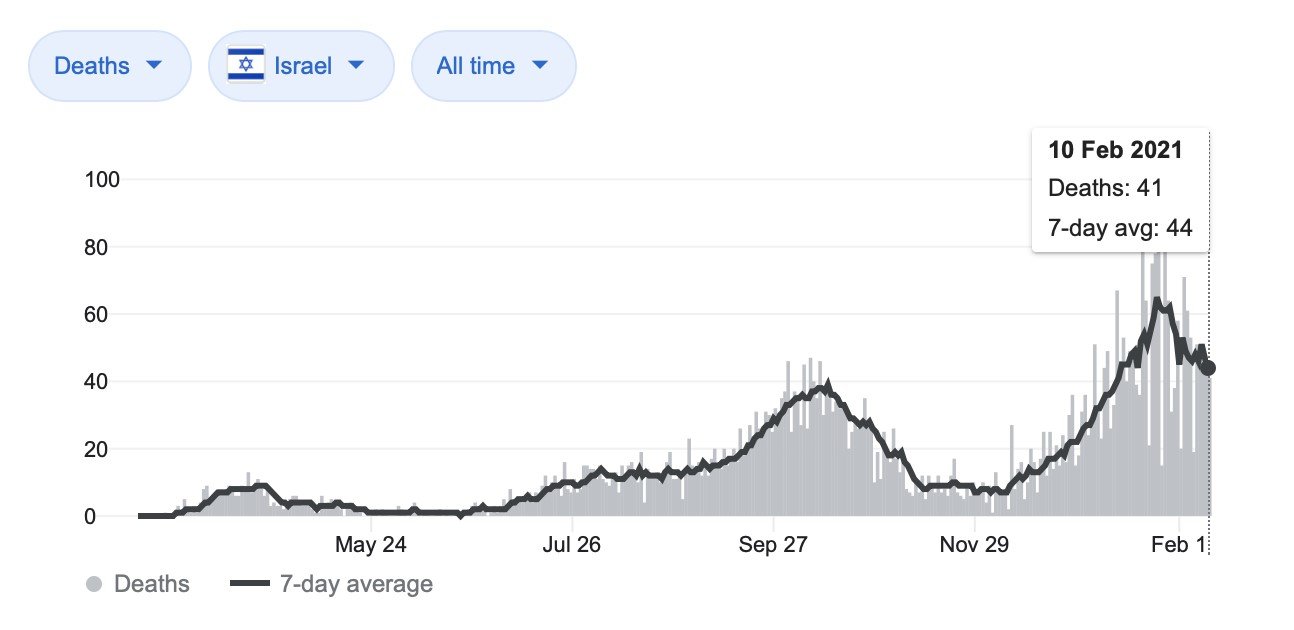
කෙසේ වෙතත්, ඒ අතරම, ඊශ්රායලය සිය තුන්වන රැල්ල හා විශාලතම මරණ අනුපාතය (5) ජනවාරි 5වන දිනට පසුව ආරම්භ කළ බව පෙනේ. ඉතින් එයින් අදහස් කරන්නේ කුමක්ද?